
Research - International Journal of Medical Research & Health Sciences ( 2023) Volume 12, Issue 1
Clinical Study of Cardiac Autonomic Dysfunction and QT Dispersion in Newly Diagnosed HIV Positive Individuals and its Correlation with CD4 Count
Keerthi Kumar1, Sandhya Rani B2*, Sindhu Kumar2 and Prathvi Nandalike22Department General Medicine, Adichunchanagiri Institute of Medical Sciences, Karnataka, India
Sandhya Rani B, Department General Medicine, Adichunchanagiri Institute of Medical Sciences, Karnataka, India, Email: Sandhya.sandy93@gmail.com
Received: 09-Dec-2022, Manuscript No. ijmrhs-22-82969; Editor assigned: 14-Dec-2022, Pre QC No. ijmrhs-22-82969 (PQ); Reviewed: 19-Dec-2022, QC No. ijmrhs-22-82969 (Q); Revised: 26-Dec-2022, Manuscript No. ijmrhs-22-82969 (R); Published: 10-Jan-2023
Abstract
Background: HIV is a global pandemic with an estimated 38 million People Living with HIV (PLHIV) worldwide. Autonomic nervous dysfunction is seen more frequently in PLHIV and Cardiac autonomic dysfunction affects severely the quality of life in them. Early detection of autonomic neuropathy helps in the rehabilitation of PLHIV. Objectives: To evaluate the presence and extent of cardiac autonomic dysfunction and QT dispersion in newly diagnosed PLHIV, and To correlate autonomic with CD4 count. Method: Age and sex-matched Case-control study was conducted in the hospitals attached to Bangalore Medical College and Research Institute (BMCRI). 30 patients (15 HIV positive with AIDS and 15 HIV positive without AIDS) and 30 healthy controls who gave consent for the study and satisfied the inclusion and exclusion criteria were enrolled in the study. Cardiac autonomic function was assessed by Ewing’s battery of autonomic function tests and QT dispersion was measured. Statistical analysis was performed using SPSS software for Windows and a p-value <0.05 was considered significant. Results: Abnormal cardiac autonomic function was observed in 20% of patients with AIDS and 6.6% of patients without AIDS. There was statistically significant differences observed between PLHIV and controls for systolic blood pressure fall on standing (p=0.02), heart rate response to deep breathing (p=0.017), to standing(p=0.004), and to Valsalva maneuver(p=0.035). 33.3% of PLHIV had abnormal QT dispersion. Conclusions: Increase in the severity of cardiac dysautonomia was seen as the CD4 counts reduced to <200 cells/microL.QT dispersion is an important predictor of cardiac autonomic dysfunction. Autonomic function tests should be performed for early detection of cardiac dysautonomia which is an important contributor to mortality and morbidity in PLHIV.
Keywords
HIV, AIDS, QT dispersion, Autonomic dispersion
Introduction
HIV is a global pandemic with currently 38.0 million PLHIV, 1.7 million people became newly infected with HIV and 0.69 million people died from AIDS-related illnesses in 2019 [1]. By the end of June 2020 estimate, 26.0 million PLHIV were accessing Antiretroviral Therapy (ART). A total of 75.7 million people have become infected with HIV since the beginning of the epidemic among which 32.7 million people have died because of AIDS-related illnesses since the start. India has the third largest HIV epidemic in the World with a prevalence of 0.22% and 2.1 million PLHIV as of 2017 [2]. In 2017 about 79% of PLHIV were aware of their status among which 71% were on ART. Karnataka has around 0.47% prevalence with about 2.47 lakh people affected by HIV as per the NACO report in 20182. Unlike other illnesses, HIV affects most commonly young adults causing great challenges in the field of social, health, and economic development. In 2019, HIV is the 19th leading cause of death worldwide and in low-income countries it is the 9th leading cause of death [3].
HIV and Autonomic Neuropathy
Autonomic dysfunction is common among HIV-infected individuals and with greater severity in patients with AIDS, usually occurring as part of a more generalized neuropathic process including distal symmetric polyneuropathy [4,5]. Clinical features of autonomic dysfunction in HIV-infected patients include presyncope, syncope, dry eyes or mouth, cold distal extremities, nausea or vomiting especially with meals, diminished sweating, diarrhea, constipation, urinary incontinence, and sexual dysfunction [6]. Subclinical autonomic neuropathy has been found in up to 50% of HIV-infected patients but various studies have reported the prevalence of autonomic nervous system dysfunction from 5% to 77% [7].
CD4 Cell Count Decline
The rate of CD4 count decline is proportional to viral burden. In a study conducted in West Africa the CD4 count decreased on average by 4% per year per log copies/mL of HIV RNA [8]. The rate of CD4 cell count decrease is also influenced by the HIV subtype or host genetic background [9]. In a large prospective study of patients with well-estimated dates of HIV infection (The Concerted Action on Seroconversion to AIDS and Death in Europe, or CASCADE cohort), the estimated median time from infection to CD4 cell count declined to <500 cells/microL was 1.19 years [10]. The faster decrease in CD4 counts in the initial stages of HIV infection reflects the destruction of CD4 cells or a shift of CD4 cells from peripheral blood to lymphoid tissue. After one year of infection the CD4 cell count decline in the range of 30 cells/microL to 90 cells/microL (average 50 cells/microL decline per year) [11,12].
QT Dispersion
A Dutch physician, William Einthoven introduced the ECG and ‘PQRST’ designations that are used today, and the ‘QT interval’ represents ventricular electrical activities, period of global ventricular depolarization, and subsequent repolarization. Newcastle proposed that the inter-lead QT interval differences within a 12-lead ECG might reflect the regional differences in myocardial refractoriness and thus recovery time and this might predict the chances of cardiac dysrhythmias [13,14]. Thus QT dispersion best represents the heterogeneity in ventricular repolarization
QT Dispersion Measurement
QT dispersion is defined as the difference between the maximum (QT max) and minimum (QT min) QT interval within the 12-lead ECG. Each of the twelve QT intervals should be calculated to determine QT dispersion. Since QT interval varies depending on heart rate, corrected QT interval can be calculated using Bazett’s formula and the difference between corrected QTc max and QTc min gives the QTc dispersion.
Measurement of the QT interval is from the beginning of the Q-wave to the end of the T-wave under normal circumstances. When the morphology of the T-wave is abnormal or when a U-wave is present, the end of the Twave is defined at the intersection of an extrapolated line of the downward slope of the T-wave to the iso-electric line, and the nadir between the T-wave and U-wave [15].
Methods
The present study was conducted on patients attending outpatient departments/admitted to the Department of Medicine of Hospitals affiliated with Bangalore Medical College and Research Institute, Bangalore.
Study Design
Case-control study.
Study Period
November 2019-May 2021
Inclusion Criteria
• Age aged more than 18 years.
• Patients who are willing to participate in the proposed study after taking Informed written consent.
• Newly detected HIV seropositive patients
Exclusion Criteria
• Patients aged below 18 years.
• History of Cardiovascular disease before testing.
• Very ill patients are unable to perfor
• Patients with Diabetes Mellitus
• Patients who are known as Alcoholics.
• Patients on Antiretroviral therapy
Sample Size
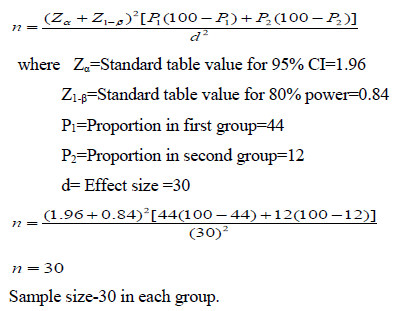
Based on a previous study by M Mahesh and M Shashidhar, 44% had abnormal heart rate variability to standing and in control was 12% and assuming the minimum expected difference will be 30%.
The sample size calculation is:
Methodology of Data Collection
The Study is a Hospital based Case-control study conducted between November 2019 to May 2021 in hospitals attached to BMCRI. After obtaining ethical clearance and approval from the Institutional Ethics Committee of BMCRI, Written informed consent was taken from the patients. Demographic profile, clinical examination, and investigations done and data collected using a study proforma for all patients.
QT dispersion was measured, and QT dispersion was determined by subtracting the minimum QT interval (QT min) from the maximum QT interval (QT max) using Standard Electrocardiogram.
Following maneuvers (Ewing battery of autonomic function tests) will be performed.
• Heart rate response to standing from a supine position.
• Heart rate variation to deep breathing.
• Heart rate response to Valsalva maneuver.
• Systolic blood pressure response to standing.
• Diastolic blood pressure response to persistent handgrip.
Statistical analysis was performed using SPSS software. Data were analyzed by descriptive statistics. Student’s t-test and Chi-square analysis were used for significant difference between the two means.
Results
The mean age in our study of 30 patients in the case group is 40.26 and in the control group is 32.23. The standard deviation in our group of cases is 12.53 whereas in the control group is 11.2. The majority of patients are in the age group between 26 years to 45 years which is an economically productive age group (Table 1).
| Age (in years) | Case group | Control group | Total |
|---|---|---|---|
| 15-25 | 3 (10%) | 11 (36.6%) | 14 (23.3%) |
| 26-35 | 10 (33.3%) | 9 (30%) | 19 (31.6%) |
| 36-45 | 7 (23.3%) | 6 (20%) | 13 (21.6%) |
| 46-55 | 7 (23.3%) | 3 (10%) | 10 (16.6%) |
| 56-65 | 3 (10%) | 1 (3.3%) | 4 (6.6%) |
| Total | 30 (100%) | 30 (100%) | 60 (100%) |
In both case and control group males are predominantly affected with 21 in number and 9 females affected with a male: female ratio of 7:3.
Our study had the majority of AIDS patients with CD4 count <50 cells/microL and the HIV-positive group had CD4 counts in the range of 401-500 (Table 2)
| CD4 count (cells/microL) | HIV-positive patients with AIDS | HIV-positive patients without AIDS |
|---|---|---|
| 0 to 50 | 11 | 0 |
| 51 to 100 | 1 | 0 |
| 101 to 200 | 3 | 0 |
| 201 to 300 | 0 | 2 |
| 301 to 400 | 0 | 2 |
| 401 to 500 | 0 | 6 |
| 501 to 600 | 0 | 3 |
| >600 | 0 | 2 |
The heart rate variation to standing results analyzed between the groups showed that there is a statistically significant difference (p-value=0.004) between HIV positive with/without AIDS patients group and the control group (Table 3).
| Heart rate response to Standing | HIV-positive with AIDS | HIV-positive without AIDS | Control group | Total |
|---|---|---|---|---|
| Normal | 7 | 13 | 29 | 49 |
| Borderline | 7 | 2 | 1 | 10 |
| Abnormal | 1 | 0 | 0 | 1 |
| Total | 15 | 15 | 30 | 60 |
| Valsalva ratio | ||||
| Normal | 4 | 6 | 24 | 34 |
| Borderline | 7 | 8 | 6 | 21 |
| Abnormal | 4 | 1 | 0 | 5 |
| Total | 15 | 15 | 30 | 60 |
Calculated Chi-square =18.55, the p-value is 0.035 and the result is significant at p<0.05 |
||||
Chi-square =17.52, the p-value is 0.004, and the result is significant at p<0.05. |
||||
The results of the Valsalva ratio are analyzed and it is found that there is a statistically significant difference between HIV positive with/without AIDS group and the control group (p-value <0.05).
The heart rate response to deep breathing results analyzed between the groups showed that there is a statistically significant difference (p-value=0.017) between HIV positive with/without AIDS patients group and the control group (Table 4).
| Heart rate response to deep breathing | HIV-positive with AIDS | HIV-positive without AIDS | Control group | Total |
|---|---|---|---|---|
| Normal | 3 | 5 | 21 | 29 |
| Borderline | 3 | 3 | 3 | 9 |
| Abnormal | 9 | 7 | 6 | 22 |
| Total | 15 | 15 | 30 | 60 |
| Systolic BP response to standing | ||||
| Normal | 3 | 10 | 25 | 38 |
| Borderline | 11 | 4 | 5 | 20 |
| Abnormal | 1 | 1 | 0 | 2 |
| Total | 15 | 15 | 30 | 60 |
Calculated Chi-square =18.26, the p-value is 0.022 and the result is significant at p<0.05 |
||||
Calculated Chi-square =12.01, the p-value is 0.017 and the result is significant at p<0.05 |
||||
The results of systolic BP response to standing are analyzed and is found that there are statistically significant differences between HIV positive with/without AIDS and the control group.
The results of Diastolic BP response to sustained handgrip are analyzed and is found that there are no significant statistical differences between HIV positive with/without AIDS and the control group as the p-value is >0.05 (Table 5).
| Diastolic BP response to sustained handgrip | HIV-positive with AIDS | HIV-positive without AIDS | Control group | Total |
|---|---|---|---|---|
| Normal | 5 | 7 | 17 | 29 |
| Borderline | 6 | 8 | 11 | 25 |
| Abnormal | 4 | 0 | 2 | 6 |
| Total | 15 | 15 | 30 | 60 |
Calculated Chi-square=7.82, the p-value is 0.22 and the result is not significant at p<0.05 |
||||
About 40% of HIV patients had resting tachycardia with a heart rate >100/min whereas only 3% of patients had resting tachycardia in the control group. This shows the abnormal cardiac sympathetic activation in HIV patients compared to the control group (Table 6).
| Heart rate | HIV-positive with AIDS | HIV-positive without AIDS | Control group |
|---|---|---|---|
| >100/min | 8 (53.3%) | 4 (26.6%) | 1 (3.4%) |
| <100/min | 7 (46.6%) | 11 (73.3%) | 29 (96.6%) |
Calculated Chi-sequare=15.02, the p-value is 0.005 and the result is significant at p<0.05 |
|||
These results showed that the majority of abnormal results are seen in CD4 counts <200 cells/microL but the difference is not statistically significant (p-value0.52). There is a negative correlation between cardiac autonomic dysfunction score and CD4 count (r=0.47) (Table 7).
| Cardiac Autonomic function (no. of patients) | CD4 cell count (cells/microL) | Total | ||
|---|---|---|---|---|
| <200 | 200-400 | >400 | ||
| Abnormal | 3 | 1 | 0 | 4 |
| Borderline | 10 | 2 | 6 | 18 |
| Normal | 2 | 1 | 5 | 8 |
| Total | 15 | 15 | 30 | |
Calculated Chi-square=5.06, the p-value is 0.52 and the result is not significant at p<0.05 |
||||
Abnormal QT dispersion is seen in 33.3% of HIV-infected patients and there is a statistically significant difference between HIV positive with/without AIDS group and the control group (p-value=0.01) (Table 8).
| QT dispersion | HIV-positive with AIDS | HIV-positive without AIDS | Control group | Total |
|---|---|---|---|---|
| Normal | 10 | 10 | 29 | 49 |
| Abnormal | 5 | 5 | 1 | 11 |
| Total | 15 | 15 | 30 | 60 |
Calculated Chi-square=9.02, the p-value is 0.01 and the result is significant at p<0.05 |
||||
Abnormalities in QT dispersion is seen in all range of CD 4 counts but an increase in number is seen in CD4 below 200 cells/microL and there is no statistical significance between QT dispersion and CD4 count(p-value>0.05) (Table 9).
| QT dispersion | CD4 cell count (cells/microL) | Total | ||
|---|---|---|---|---|
| <200 | 200-400 | >400 | ||
| Normal | 10 | 1 | 9 | 20 |
| Abnormal | 5 | 3 | 2 | 10 |
| Total | 15 | 15 | 30 | |
Calculated Chi-square=4.26, the p-value is 0.1 and the result is not significant at p<0.05 |
||||
Discussion
In the present Prospective age-sex matched case-control study, HIV patients attending the Department of Medicine, Bangalore Medical College, and Research Institute were evaluated clinically to study the presence and extent of Cardiac autonomic dysfunction and QT dispersion. The correlation of Cardiac autonomic dysfunction with CD4 counts was studied. The observation and results of the present study are compared with other studies and discussed as follows.
Age Distribution
In the current study, the age of the study population constituted 19 years-65 years, with the mean age of the case group being 40.26 ± 12.53 years and the mean age of the control group being 32.23 ± 11.2 years. The age group in our study can be comparable to the study conducted by which had a similar study design with observations showing an age range of 26 years-60 years in the study, the mean age of the case group was 38 years, and the mean age of the control group was 38.12 years. It was also comparable to a study conducted on the Indian population showing the mean age of patients in the study group, was 35.08 ± 8.2 years and that of the control group was 35.12 years ± 8.6 years [16].
Sex Distribution
In the current study majority of cases and controls were males (70%) compared to females (30%). The male-tofemale ratio is 2.3:1 in our study. A similar kind of male preponderance was consistent with other. A similar kind of sex distribution was also seen in the study by Utsav Kumar Sahu et al18 which had male to female ratio of 2.3:1 [17,18].
Resting Heart Rate
In the present study resting heart rate of greater than 100 beats/min suggesting resting tachycardia was observed in 53.3% of the AIDS group and 26.6% of the HIV-positive group. This shows the abnormality in cardiac parasympathetic activity causing the unopposed sympathetic drive to the heart resulting in tachycardia. This finding was consistent which showed resting heart rate was significantly higher in PLHIV compared to controls [19,20].
Ewing’s Battery of Autonomic Function Tests
Heart rate response to deep breathing: In the present study, heart rate response to deep breathing in HIVpositive with AIDS showed abnormal results in 60% of cases and borderline values in 20% of cases. HIVpositive without AIDS had 46.6% with abnormal values, and borderline dysfunction was seen in 20% of cases. Similar kind of observations was noted in a study, where AIDS cases had 56% abnormal dysfunction, and 24% borderline dysfunction whereas HIV cases showed 40% abnormal values and 24% borderline dysfunction. Similar kind of results with an increase in abnormal dysfunction in AIDS cases (48%) compared with HIV cases [16].
Heart rate response to standing: In the present study, heart rate response to standing in HIV positive with AIDS showed 6.6% abnormal values, and 46.6% borderline values whereas HIV positive without AIDS had 13.3% cases with borderline dysfunction, and this heart rate variation to standing between HIV/AIDS group and the control group was statistically significant. Observed a significant difference in this test between the HIV group and the control group [17].
Heart rate response to Valsalva maneuver: In the current study, the Valsalva ratio was abnormal in 26.6% and borderline dysfunction in 46.6% among AIDS cases, however, HIV cases without AIDS had 6.6% abnormal and 53.3% with borderline results. And the Valsalva ratio was found to be statistically significant among HIV/ AIDS group and the control group. Similar result of significant differences in the Valsalva ratio between HIV positive with/without AIDS and the Control group [19,21].
Systolic blood pressure response to standing: In our study, a fall in Systolic blood pressure to standing was abnormal in 6.6% and borderline results in 73.3% of AIDS cases. In HIV cases it was observed 6.6% abnormal results and 26.6% borderline results among HIV cases. The results of systolic BP response to the standing analysis found that there is a significant statistical difference between HIV positive with/without AIDS and the control group. Similar observations of an 8% abnormality of fall in systolic BP on standing in HIV with found to have significant differences in systolic BP response to standing among HIV with/without AIDS and the control group [16,18].
Diastolic blood pressure response to persistent handgrip: In the present study diastolic BP response to sustained handgrip was found to have 26.6% abnormal results and 40% borderline results among AIDS cases. 6.6% of abnormality and 53.3% of borderline dysfunction were noted n HIV cases. However, there was no significant statistical difference between the HIV ± AIDS group and the control group. Found no statistical difference between HIV with or without AIDS group and the control group in this test [18]. However, statistically significant difference in the increase of diastolic BP to sustained handgrip among the HIV with or without AIDS group and control group [16,21].
The results of the present study correlated with a study. The present study suggested that autonomic dysfunction occurs in cases of AIDS and also in the early course of HIV infection but increased severity of dysfunction was noted in AIDS patients. Autonomic neuropathy was frequently found in HIV-infected patients and that AIDS is associated with more severe dysfunction [22].
Correlation of CD4 count with Cardiac autonomic dysfunction:
In the present study, cardiac autonomic dysfunction was seen at a wide range of CD4 counts, and the majority of abnormal results were seen in CD4 counts <100 cells/microL but the results were statistically insignificant. It had a similar result with more abnormal results found below the CD4 range and the difference was not statistically significant. The majority of abnormal values in less than 200 CD4 counts [16,18].
QT dispersion and its correlation with CD4 count: In the present study abnormal QT dispersion was seen in 33.3% of HIV-infected patients and the result had a statistically significant difference (p<0.05) between the HIV ± AIDS group and control group. The same observations were made by Utsav Kumar Sahu et al., and Mahesh M et al., where the majority of abnormality in cardiac autonomic function was seen below CD4 cunt of 200 cells/microL
Conclusion
Cardiac autonomic dysfunction is a common and clinically relevant problem in HIV-infected patients. The severity of dysfunction is aggravated by an increase in the severity of the disease and a reduction in CD4 count. When HIV-infected individuals present with common complaints of dizziness, impotence, and bowel and bladder dysfunction, a simple cost-effective bedside Ewing’s battery of autonomic function tests can be conducted to know the presence of Cardiac autonomic dysfunction. Reduced heart rate variability is the most common manifestation found in Cardiac autonomic dysfunction in PLHIV
QT dispersion is a simple ECG parameter suggesting the repolarization abnormality of ventricles and represents a predictor of Cardiac autonomic dysfunction. An increase in the severity of Cardiac dysautonomia correlates with QT dispersion.
Some of the antiretroviral drugs are also capable of causing autonomic dysfunction. The early detection of cardiac autonomic dysfunction in newly diagnosed PLHIV helps in taking appropriate therapeutic measures to prevent morbidity and mortality due to cardiac events in PLHIV.
Declarations
Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
None
Ethical approval:
Institutional ethical committee clearance taken
References
- Global HIV & AIDS statistics-2020 fact sheet
- HIV facts and figures, "National AIDS Control Organization, MoHFW", GoI, 2020.
- National AIDS Control Organization, MoHFW
- Becker, Klaus, et al. "Characterization and natural course of cardiac autonomic nervous dysfunction in HIV-infected patients." Aids, Vol. 11, No. 6, 1997, pp. 751-57.
Google Scholar Crossref - Robinson-Papp, Jessica, et al. "Autonomic dysfunction is common in HIV and associated with distal symmetric polyneuropathy." Journal of neurovirology, Vol. 19, No. 2, 2013, pp. 172-80.
Google Scholar Crossref - Sletten, David M., et al. "COMPASS 31: a refined and abbreviated Composite Autonomic Symptom Score." Mayo Clinic Proceedings, Vol. 87, No. 12, 2012, pp. 1196-01.
Google Scholar Crossref - Badiger, Sharan, Prema T. Akkasaligar, and Deepak Kadeli. "Human Immunodeficiency Virus Infection and Cardiac Autonomic Neuropathy." International Scholarly and Scientific Research and Innovation, Vol. 11, 2017.
Google Scholar Crossref - Gottlieb, Geoffrey S., et al. "Equal plasma viral loads predict a similar rate of CD4±T cell decline in human immunodeficiency virus (HIV) type 1-and HIV-2-infected individuals from Senegal, West Africa." The Journal of infectious diseases, Vol. 185, No. 7, 2002, pp. 905-14.
Google Scholar Crossref - Mlisana, Koleka, et al. "Rapid disease progression in HIV-1 subtype C–infected South African Women ." Clinical Infectious Diseases, Vol. 59, No. 9, 2014, pp. 1322-31.
Google Scholar Crossref - Lodi, Sara, et al. "Time from human immunodeficiency virus seroconversion to reaching CD4+ cell count thresholds< 200,< 350, and< 500 cells/mm3: assessment of need following changes in treatment guidelines." Clinical infectious diseases, Vol. 53, No. 8, 2011, pp. 817-25.
Google Scholar Crossref - Schacker, Timothy W., et al. "Biological and virologic characteristics of primary HIV infection." Annals of internal medicine, Vol. 128, No. 8, 1998, pp. 613-20.
Google Scholar Crossref - Hughes, Michael D., et al. "Within-subject variation in CD4 lymphocyte count in asymptomatic human immunodeficiency virus infection: implications for patient monitoring." Journal of Infectious Diseases, Vol. 169, No. 1, 1994, pp. 28-36.
Google Scholar Crossref - Waller, Augustus D. "A demonstration on man of electromotive changes accompanying the heart's beat." The Journal of physiology, Vol. 8, No. 5, 1887, pp. 229-34.
Google Scholar Crossref - Day, Christopher P., Janet M. McComb, and R. W. Campbell. "QT dispersion: an indication of arrhythmia risk in patients with long QT intervals." Heart, Vol. 63, No. 6, 1990, pp. 342-44.
Google Scholar Crossref - Rogstad, Karen E., et al. "Cardiovascular autonomic neuropathy in HIV infected patients." Sexually transmitted infections, Vol. 75, No. 4, 1999, pp. 264-67.
Google Scholar Crossref - Mahesh, M., and M. Shashidhara. "Evaluation of Cardiac Autonomic Dysfunction in Human Immunodeficiency Virus Infection and its Correlation with CD4 Levels." International Journal of Scientific Study, Vol. 3, No. 12, 2016, pp. 268-73.
Google Scholar - Sashindran, V. K., et al. "Cardiac Autonomic Dysfunction in Human Immunodeficiency Virus Infected Patients: A Cross Sectional Study." Journal of AIDS and Clinical Research, Vol. 10, No. 783, 2019, p. 2.
Google Scholar - Sahu, Utsav Kumar, and Maniram Kumhar. "Clinical Study of Cardiac Autonomic Dysfunction and QT Dispersion in Newly Diagnosed HIV/AIDS Patients and its Correlation with CD (4) Count." The Journal of the Association of Physicians of India, Vol. 66, No. 5, 2018, pp. 66-68.
Google Scholar - Badiger, Sharan, Prema T. Akkasaligar, and Deepak Kadeli. "Human Immunodeficiency Virus Infection and Cardiac Autonomic Neuropathy." 2017.
Google Scholar Crossref - Becker, Klaus, et al. "Characterization and natural course of cardiac autonomic nervous dysfunction in HIV-infected patients." Aids, Vol. 11, No. 6, 1997, pp. 751-57.
Google Scholar Crossref - Nzuobontane, Divine, Blackett Kathleen-Ngu, and Kuaban Christopher. "Cardiovascular autonomic dysfunction in Africans infected with human immunodeficiency virus." Journal of the Royal Society of Medicine, Vol. 95, No. 9, 2002, pp. 445-47.
Google Scholar Crossref - Rüttimann, Sigmund, et al. "High frequency of human immunodeficiency virus-associated autonomic neuropathy and more severe involvement in advanced stages of human immunodeficiency virus disease." Archives of internal medicine, Vol. 151, No. 12, 1991, pp. 2441-43.
Google Scholar Crossref